Depending on viewing angle: We might observe nothing more than an artefact of measuring antibodies.
If we assume that not all patients form antibodies at the same incidence rate but all patients with the same probability and one and same patient at a constant rate then a quite simple effect of immunogenicity might be observed:
in constant administration antibodies are just used up at a constant rate, being active and bound, but not free and measurable. In episodic treatment the rate of antibody production then leads to more free antibodies (not used up) to measure – and immediately available for action against the biologic, once that is re-introduced to the system.
Thus a simple rephrasing of the introductory quote from the question might read
Interruption of scheduled maintenance anti-TNF therapy or episodic therapy has consistently been associated with higher rates of antibody formation detection.
A recent paper summarises the situation as:
Treatment options include biologic therapies; however, a proportion of patients lose response to biologics, partly due to the formation of anti-drug antibodies (ADAbs). Concomitant immunosuppressive agents reduce the development of ADAbs.
A comprehensive literature search was conducted for articles published January 2009 to August 2015 reporting immunogenicity to adalimumab (ADM), certolizumab pegol (CZP), golimumab, infliximab (IFX), ustekinumab, and vedolizumab in inflammatory bowel disease (IBD).
In most of the included studies that evaluated efficacy, the presence of ADAbs was associated with a reduction in efficacy. Efficacy was assessed in a variety of ways, including Crohn’s Disease Activity Index (CDAI) response/remission, Mayo response, endoscopic improvement and treatment discontinuation. In studies of IFX, the proportion of patients achieving and maintaining a response was generally lower for patients with detected ADAbs than those without detected ADAbs ( Supplementary Table 7). ADAbs to ADM were also associated with reduced efficacy and a loss of response, together with a high rate of secondary treatment failure; these associ-ations were shown to be statistically significant in some studies ( Supplementary Table 8). In one study,26 discontinuation of ADM treatment was reported to be very high (83.3%) in patients with ADAbs ( Supplementary Table 8).
The timing of sampling (prior to or just after the next administration) greatly influences the detection rate. Most assays do not detect ADAbs in the presence of drug; since drug concentration is the lowest just before the next infusion, this is the optimal time to sample. This might be one explanation for the formation of ADAbs being reported to be lower in RCTs than in observational studies. Often, a limited number of time points were studied, and insufficient time was allowed for drug levels to decrease prior to sampling. However, it is also likely that improved assay techniques used in observational studies, together with the selection of patients with loss of response, led to higher levels of detection of ADAbs than in RCTs.
Séverine Vermeire & Ann Gils & Paola Accossato & Sadiq Lula & Amy Marren: "Immunogenicity of biologics in inflammatory bowel disease", Therap Adv Gastroenterol. 2018; 11: 1756283X17750355. Published online 2018 Jan 21. doi: 10.1177/1756283X17750355, PMCID: PMC5784568, PMID: 29383030.
The above is just hopefully informed speculation, though, based on the lack of information in the studied papers as to how antibodies were measured. That is whether all of these possible values were taken: antigen concentration, the antigen-antibody complex concentration, the free antibody and/or total antibody concentrations.
The antigen-antibody reaction is widely used in laboratory diagnostics, including immunohaematology. It is a reversible chemical reaction:
antigen + antibody ⇄ antigen - antibody complex
The forces joining the antigen-antibody complex are not strong covalent bonds but weaker bonds, appropriately named “weak interactions”.
Roberto Reverberi & Lorenzo Reverberi: "Factors affecting the antigen-antibody reaction", Blood Transfus. 2007 Oct; 5(4): 227–240. doi: 10.2450/2007.0047-07 PMCID: PMC2581910, PMID: 19204779
Chasing a wild goose: Even more speculative might be the thought that in these processes an effect of continuous reinforcement versus intermittent reinforcement occurs.
One point to observe: Infliximab is quite different to other anti-TNF agents, as they are quite different in their attributes:
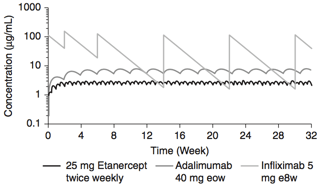
A pharmacokinetics simulation of serum concentrations of infliximab, etanercept, and adalimumab at steady state in patients with RA treated with each drug at doses and schedules shown.
Clinical consequences of immunogenicity of TNF antagonists include acquired drug resistance and infusion or injection site reactions. Anti-drug antibodies can form multivalent complexes with the target drug, leading to rapid clearance and inactivation of the drug. Strategies to deal with this include dose escalation or the addition of concomitant immunosuppressive therapy to reduce antibody formation. Studies of the immunogenicity of protein-based drugs have suggested that chimeric antibodies are generally more immunogenic than humanized or human antibodies. However, comparisons of the immunogenic potential of the anti-TNF agents are difficult, largely because of differences in the sensitivity of the assays designed to detect anti-drug antibodies, as well as the interference in the assays of the drug itself.
Jennifer L. Jones: "Are all anti-TNF agents the same?", in: Peter M. Irving et al (Eds): "Clinical Dilemmas in Inflammatory Bowel Disease", Wiley-Blackwell: Chichester, Hobokem 22011.