I was referred to a Rheumatologist earlier this year due to all my symptoms: constant fatigue, getting sick all the time by every little thing, having unexplained fevers, having constant joint pain, swollen joints, digestive issues, nausea, sensitivity to light, erratic menstruation cycles, chest pain, uptick in my migraines, being in a brain fog, coldness in extremities, etc. I already had been diagnosed with fibromyalgia and osteoarthritis, but my Dr. was suspicious that I might I have Lupus so he ordered an ANA (antinuclear antibody) test.
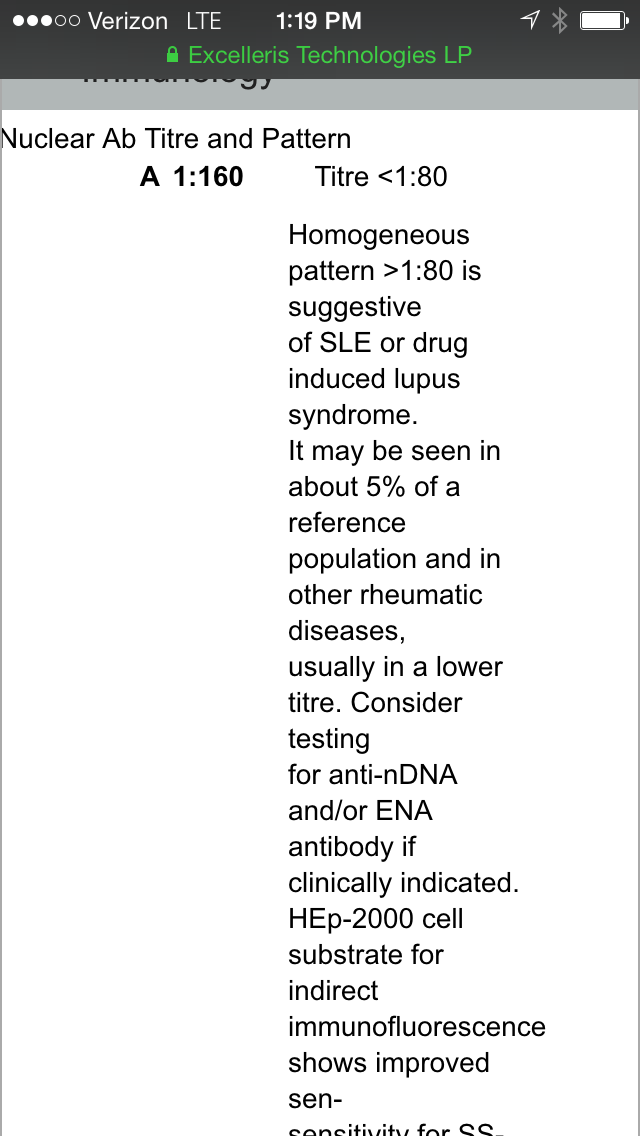
My test result is seen below: Abnormal 1:160. My WBC was also soaring, but, my Dr. was undecided on whether or not to diagnose me with Lupus -- though the laboratory technicians had recommended the diagnosis.
So is a positive 1:160 ANA test result still considered ambiguous for diagnosis Lupus? He labeled me border-line Lupus. Is that a real thing? What other diagnostic testing is needed to diagnosis definitively that I have or do not have Lupus?
Or should I see a different rhematologist?
{kind=link}