Regarding the steps, I'll get to #1 a bit later. It's actually a bit subtle how mRNA vaccines work in re #2, i.e. actually making sure translation happens. It also makes sense to discuss this first; otherwise, there's not much point in delivering something that doesn't work. A popsci explanation "from the helicopter" is that one needs to use "modified nucleosides" to begin with:
The stumbling block, as Karikó’s many grant rejections pointed out, was that injecting synthetic mRNA typically led to that vexing immune response; the body sensed a chemical intruder, and went to war. The solution, Karikó and Weissman discovered, was the biological equivalent of swapping out a tire.
Every strand of mRNA is made up of four molecular building blocks called nucleosides. But in its altered, synthetic form, one of those building blocks, like a misaligned wheel on a car, was throwing everything off by signaling the immune system. So Karikó and Weissman simply subbed it out for a slightly tweaked version, creating a hybrid mRNA that could sneak its way into cells without alerting the body’s defenses.
“That was a key discovery,” said Norbert Pardi, an assistant professor of medicine at Penn and frequent collaborator. “Karikó and Weissman figured out that if you incorporate modified nucleosides into mRNA, you can kill two birds with one stone.”
And the more in-depth version of that, from a review
Enzymatically synthesized mRNA preparations contain double-stranded RNA (dsRNA) contaminants as
aberrant products of the IVT reaction. As a mimic of
viral genomes and replication intermediates, dsRNA is
a potent pathogen-associated molecular pattern (PAMP)
that is sensed by pattern recognition receptors in multiple cellular compartments [...]. Recognition of IVT
mRNA contaminated with dsRNA results in robust
type I interferon production, which upregulates the
expression and activation of protein kinase R (PKR; also
known as EIF2AK2) and 2'-5'-oligoadenylate synthetase
(OAS), leading to the inhibition of translation and the
degradation of cellular mRNA and ribosomal RNA respectively. Karikó and colleagues have demonstrated
that contaminating dsRNA can be efficiently removed
from IVT mRNA by chromatographic methods such as
reverse-phase fast protein liquid chromatography (FPLC)
or high-performance liquid chromatography (HPLC).
Strikingly, purification by FPLC has been shown to
increase protein production from IVT mRNA by up
to 1,000-fold in primary human DCs. Thus, appropriate purification of IVT mRNA seems to be critical for
maximizing protein (immunogen) production in DCs
and for avoiding unwanted innate immune activation.
Besides dsRNA contaminants, single-stranded mRNA
molecules are themselves a PAMP when delivered to
cells exogenously. Single-stranded oligoribonucleotides
and their degradative products are detected by the endosomal sensors Toll-like receptor 7 (TLR7) and TLR8, resulting in type I interferon production.
Crucially, it was discovered that the incorporation of
naturally occurring chemically modified nucleosides,
including but not limited to pseudouridine and
1-methylpseudouridine, prevents activation of TLR7,
TLR8 and other innate immune sensors, thus reducing type I interferon signalling. Nucleoside modification
also partially suppresses the recognition of dsRNA species. As a result, Karikó and others have shown that
nucleoside-modified mRNA is translated more efficiently
than unmodified mRNA in vitro, particularly in primary
DCs, and in vivo in mice. Notably, the highest level of
protein production in DCs was observed when mRNA
was both FPLC-purified and nucleoside-modified.
In other words, the mRNA gets "blown to bits" by the immune system before much translation, unless you're "really clever" how you introduce it, i.e. sans dsRNA contaminants (that are alas actually quite easy to produce) and with nucleoside-modification pseudouridine / 1-methylpseudouridine. If you look at the wiki article for pseudouridine, you'll see that it's naturally occurring in RNA, but it is rare. (It's actually a good question whether it is this relative rarity in nature that (evolutionary) has made the immune system not PAMP-react strongly to the pseudouridine-modified mRNA so that it can "sneak in" and get translated, instead of being mostly destroyed before translation. Alternatively or additionally, there's also the fact that pseudouridine seems to act as a more potent version of uridine.)
As far step #1 is concerned, "naked" mRNA doesn't survive for long in the extracellular space because of the "omnipresence of extracellular ribonucleases". On top of that, mRNA from extracellular space is not take up effectively by the cells due to its "hydrophilicity and strong net negative charge". So some kind of wrapper/vehicle that basically emulates a virus' envelope is needed. Various techniques/envelopes have been tried, but to keep this simple (and relevant to Covid vaccines currently approved), it's the LNP (lipid nano-particle) method that has been used most successfully:
Lipid nanoparticles (LNPs) have
become one of the most appealing and commonly used
mRNA delivery tools. LNPs often consist of four components:
an ionizable cationic lipid, which promotes
self-assembly into virus-sized (~100 nm) particles and
allows endosomal release of mRNA to the cytoplasm;
lipid-linked polyethylene glycol (PEG), which increases
the half-life of formulations; cholesterol, a stabilizing
agent; and naturally occurring phospholipids, which
support lipid bilayer structure. Numerous studies
have demonstrated efficient in vivo siRNA delivery
by LNPs [...], but it has only recently
been shown that LNPs are potent tools for in vivo delivery
of self-amplifying RNA and conventional, non-replicating
mRNA. Systemically delivered mRNA–LNP
complexes mainly target the liver owing to binding of
apolipoprotein E and subsequent receptor-mediated
uptake by hepatocytes, and intradermal, intramuscular
and subcutaneous administration have been shown
to produce prolonged protein expression at the site
of the injection. The mechanisms of mRNA escape
into the cytoplasm are incompletely understood, not
only for artificial liposomes but also for naturally
occurring exosomes. Further research into this area
will likely be of great benefit to the field of therapeutic
RNA delivery.
Wikipedia has an article on some variety of these LNPs.
Whether a RNA vaccine produces a more gradual immune response (than the traditional ones) is a good question (I don't know the answer off-hand), but if in "inflammation" we include allergic reactions, alas the sudden infusion of LNPs does seem to cause some such allergic reactions, although the link doesn't seem conclusive at the moment.
Anaphylactic reactions can occur with any vaccine, but are usually extremely rare—about one per 1 million doses. As of 19 December, the United States had seen six cases of anaphylaxis among 272,001 people who received the COVID-19 vaccine, according to a recent presentation by Thomas Clark of the U.S. Centers for Disease Control and Prevention.
Perhaps worth mentioning here that a naive (not using modified nucleosides) approach to RNA vaccines is basically "pain for no (or little) gain" as the response that comes with the immune-response destruction of mRNA is apparently inflammatory in its symptoms:
Ordinary mRNA produces only low levels of proteins, and the molecule degrades too quickly inside the body to make it suitable as a therapeutic. On top of that, RNA can trigger an immune response that’s independent of the response to the protein it encodes. “If you just inject foreign RNA into people or animals, you can induce a very serious inflammatory response,” Pardi [an mRNA vaccine specialist at the University of Pennsylvania] says. He adds that this is our bodies’ defense mechanism against viruses, which can use either DNA or RNA to store their genetic information.
It's unclear whether the mRNA vaccines (of the clever, i.e. modified nucleosides kind) produce less inflammatory reactions than vaccines based on entirely different technologies for the same disease, but some experts have speculated that the high efficacy observed from the Covid-19 mRNA vaccines may actually be boosted by the "usual" inflammatory response to mRNA, as these are not completely absent even in modified nucleoside vaccines:
[Margaret] Liu [the chairman of the board of the International Society for Vaccines] also hypothesizes that one explanation for the high levels of efficacy is that the vaccines might be triggering a nonspecific inflammatory response to the mRNA that could be heightening its specific immune response, given that the modified nucleoside technique reduced inflammation but hasn’t eliminated it completely. On the flip side, she adds, this may also explain the intense reactions such as aches and fevers reported in some recipients of the mRNA SARS-CoV-2 vaccines. (Others have suggested that the lipid nanoparticle is responsible for these severe, but transient, side effects reported in some trial participants.)
According to a November story in Science the Covid-19 mRNA vaccines produced more reactogencity (which includes inflammation) than typically expected in vaccines in general:
Fewer than 2% of recipients of the Pfizer and Moderna vaccines developed severe fevers of 39°C to 40°C. But if the companies win regulatory approvals, they’re aiming to supply vaccine to 35 million people globally by the end of December. If 2% experienced severe fever, that would be 700,000 people.
Other transient side effects would likely affect even more people. The independent board that conducted the interim analysis of Moderna’s huge trial found that severe side effects included fatigue in 9.7% of participants, muscle pain in 8.9%, joint pain in 5.2%, and headache in 4.5%. For the Pfizer/BioNTech vaccine, the numbers were lower: Severe side effects included fatigue (3.8%) and headache (2%).
That’s a higher rate of severe reactions than people may be accustomed to. “This is higher reactogenicity than is ordinarily seen with most flu vaccines, even the high-dose ones,” says Arnold Monto, an epidemiologist at the University of Michigan School of Public Health.
More up-to-date numbers on reactogenicity were actually the subject of another question here. (Apparently there were around 1% in a larger sample, i.e. around 3,000 cases in the 272,000 sample that was the topic of a recent CDC report.)
And contra to Liu, Weissman says it's the LNPs that cause the local reactions, not the mRNA in its modified form:
“We suspect the lipid nanoparticle causes the reactogenicity, because lipid nanoparticles without mRNA in them do the same thing in animals,” [...] “We see production, in the muscle, of inflammatory mediators that cause pain, [redness], swelling, fever, flulike symptoms, etc.”
Briefly, as far as advantages of mRNA vaccines (despite the tech challenges, only resolved fairly recently), these come from the disadvantages of other vaccine techs. For example, attenuated vaccines have more safety risks, adenovirus-platform vaccines present some risk of non-response due to anti-bodies to the vector etc. Basically mRNA vaccines produce response to a "minimal target" (also because the wrapper is synthetic "nanotech".) Although many publications (from mRNA field) only speak of this as an advantage, clearly getting the target wrong in terms of the relevant proteins can be a problem, but presumably one that is fast and easy to identify.
There is one (theoretical at least) immunological advantage to gene-based vaccines, the recruitment of the MHC-I pathway:
genetic approaches have a potential immunological advantage. In addition to eliciting antibodies and CD4+ helper T cells, they recruit CD8+ cytotoxic T cells, also known as killer T cells, through the major histocompatibility class I pathway.
According to Otto Yang, MD, an infectious disease researcher and clinician at the University of California, Los Angeles, David Geffen School of Medicine, the body’s cells only display viral proteins on their surface through this pathway if those cells themselves have produced the proteins. “If you just inject a protein or inject a dead virus, it doesn’t get into that pathway and doesn't get displayed that way, and so the T cells don’t get stimulated,” he said.
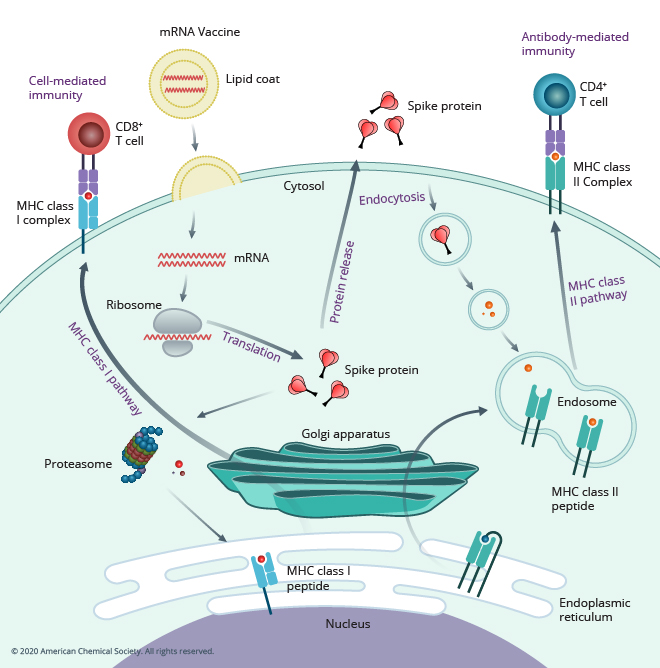
And to sorta put it all in a one picture, the ACS has this probably most informative "all in one" pictures of how mRNA vaccines work, both before and after protein release, although the diagram eschews subtleties relating to step #2 (i.e. why modified nucleosides are needed):
As far as the final quote in your question, that has more to do with how mRNA are produced (at scale), a discussion which is often eschewed in medical sources or dealt with in one sentence like "fully synthetic manufacturing process that allows production of different vaccines using the same established production process and facility". Perhaps Chemistry SE would be a better place to ask for details on the latter, i.e. how mRNA vaccines are produced and why that is an industrial advantage. (I'm not saying it's off-topic here, just that questions on the manufacturing process of medications are practically non-existent here on Med SE, especially on the industrial angle.)
On the level of generalities, and mostly with respect to (difficulties of) vaccine manufacture by non-synthetic techniques:
Vaccine manufacture is one of the most challenging industries. Even the most basic manufacturing steps necessary to produce vaccines in a manner that is safe, effective, and consistent over the life cycle of a vaccine are difficult to execute. Outcomes can vary widely due to the nearly infinite combinations of biological variability in basic starting materials, the microorganism itself, the environmental condition of the microbial culture, the knowledge and experience of the manufacturing technician, and the steps involved in the purification processes. To add to the complexity, the methods used to analyze the biological processes and antigens resulting from vaccine production often have high inherent variability. Failure to manage these risks can result in costly product recalls, and suspensions and penalties may be assessed if a manufacturer fails to fulfil supply agreements. In addition, lack of supply can disrupt routine immunization programs and negatively impact national public health outcomes.
Regulatory authorities license not only a specific biological entity, but also the processes by which that entity is produced, tested, and released for use. Subtle changes in the production process may alter the final product and change its purity, safety, or efficacy. Further, the in vitro analytics required to release the product may not detect a change in process and a clinical trial may be needed to validate a new process and to maintain licensure of a product. This compounded risk of biological and physical variability makes vaccine manufacturing more challenging than typical small molecule pharmaceuticals and is a primary root cause of the high proportion of vaccine manufacturing failures and supply shortages. This is also the main reason why the number of vaccine manufacturers that succeed and thrive remains low despite unmet demand for many vaccines globally. Moreover, individual vaccine prices do not always decline, even after the patents expire, in contrast to pharmaceutical products. In fact, many vaccine patents protect the manufacturing process rather than the antigen that is produced by the process, which is not always the analogous case for small molecule pharmaceutical products. These process patents may present a more significant barrier to entry than the patent on the vaccine composition itself.
Significant changes in the manufacturing process, such as new facilities, manufacturing equipment or changes in raw materials, will typically trigger new regulatory requirements, including clinical trials. These requirements will confirm that the vaccine is still effective and comparable to the product produced by the original vaccine process and studied in the original clinical studies. [...] Manufacturers are challenged to balance the competing goals of speed to market and process optimization; getting to market earlier increases revenue in the short term, but locking in a further optimized process may generate cost savings over the entire vaccine life-cycle.
There are many production platforms in use today and they vary widely [...] At one end [of production complexity] is live attenuated oral polio vaccine with significantly lower Cost of Goods Sold (COGS) while at the other end is the highly complex pneumococcal conjugate vaccine. While there may be common equipment across platforms such as bio reactors, filtration and chromatography equipment, filling and lyophilization equipment, the sequence of operations and the specific cycles for each product vary. In most cases, each product (or group of products within a product family) has its own dedicated facility and production team. This dedicated labor and equipment allows for flexibility to address unpredictable demand, but tends to increase costs. [...]
Facilities can cost 50–500 M USD per antigen based on the high complexity of design, automation, segregation, utilities, and contamination controls, and as much as 700 M USD for multiple vaccines. [...] The US Department of Defense estimated the 25-year life-cycle cost of a 3-product facility to be 1.56 billion USD and that 7 years are needed to design, build, validate, and commence commercial manufacturing.